Orthopedic Problems concerning the foot or the ankle, Injuries of foot or ankle.
Meniscus
In 1897 physicians believed that meniscus was the residual degenerated muscle of the knee. Only in 1937 did they understand that they were useful for the motion of the knee and the distribution of weight of the femur on the tibia. Later in 1947 they realized that menisectomy lead to premature joint knee damage.
The doctors thought that the idea of being able to look inside the human body without “opening it” was exciting. In 1809 we have the first reference on the Endoscope, which was consisted of simple pipes and was using a candle as a source of light. In 1853, the cystoscope for urinary control is mentioned for the first time and in 1919 in Japan, a cystoscope was used to control the Interior of a knee. The endoscopes which are used in orthopedics for the control of the joints are called arthroscopes. In 1962 was the first Arthroscopic menisectomy was performed. The revolution in arthroscopies took place in the last twenty years, where the Arthroscopic camcorder was used, improving-as a result- the techniques that had been used.
[dt_sc_hr]
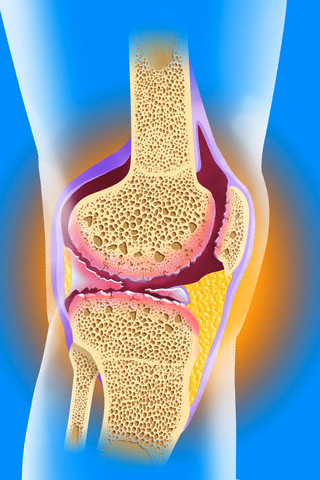
Today the arthroscopic repair of meniscal lesions is the most common orthopedic surgery. The knee is a complex anatomical articulation and menisci, which are basically two avascular cartilages, serve in normalizing body weights when walking in the knee joint.
On the flexion-extension of the joints, they move back and forward. They could be injured mainly in combination with the simultaneous bending of the knee. Such injuries are common in sports activities and especially in football.
As meniscus damage is considered to be the partial or total rupture. The lesions are divided into two major categories, the traumatic and degenerative one (arthritis). The latter is commonly found in persons between 50-60 years and is not reported as a violent knee injury. On the contrary, in the cases of traumatic raptures, we have a recent or old injury history and hydrarthus (swelling).
When I talk to my patients, I compare the ruptured meniscus with a paper cut in two. Just like the paper, when the meniscus is ruptured, it does not lose its usefulness on the knee but its quality is limited. In practice, this means that the sufferer may have a ruptured meniscus without many symptoms.
The diagnosis of the injury is always made after the patient’s history is taken and the physical examination is performed. The MRI confirms the diagnosis but its credibility varies from 70-100%. This means that the final diagnosis is always made by the doctor.
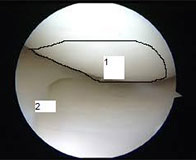
Meniscus injuries are always treated with an arthroscopic surgery through two small openings (1 cm) on the hinge and the patient returns home the same day of the operation. In most cases, the damage of the meniscus is removed except for certain cases where a suture can be done as well.
[dt_sc_pullquote type=”pullquote5″ align=”center” icon=”yes” cite=”Dr. Granitsas PhD”]My opinion is that not all menisci ruptures need to be treated with Arthroscopy. The surgery becomes necessary if the knee nuisances are frequent and persistent. If the knee shows an occasional nuisance of minor importance, then a simple muscle strengthening of the quadriceps and the biceps is probably enough.[/dt_sc_pullquote]
Between the age of 50 and 60, the meniscus rupture is usually of degenerated type. The arthroscopy in this case is not just about removing the part of the meniscus that has been damaged but mainly with the correction of the degenerative lesions of the knee (osteoarthritic), and the result will be the maintenance and preservation of the proper operation of the joint.
After the age of 60 and since the arthritic knee lesions are intense, the doctor should focus primarily on total Arthroplasty and less in Arthroscopy. Of course, even in a severe case of knee arthritis, it wouldn’t be wrong to turn to Arthroscopy, but the results wouldn’t be as satisfactory as in the group between the age of 50 and 60.
To sum up, until the age of 50, I strongly recommend the restoration of the meniscus with Arthroscopy, given that the exercises for quadriceps cannot solve the problem. Between the ages of 50 and 60, I recommend the Arthroscopy with a simultaneous correction of the degenerative lesions and over the age of 60, an Arthroplasty or Arthroscopy with the proper update of the patient over the expected result.